Residual paralysis affects up to 40% of patients without quantitative monitoring.
Learn what 0% residual paralysis looks like in clinical practice, and how TwitchView monitoring with guided reversal makes it possible.

Access Our NMB Reversal Guide PDF - Supports Reversal Drug and Dosage Decisions
The ASA House of Delegates approved practice guidelines for neuromuscular blockade in October 2022. The ASA practice guidelines, a report written by the American Society of Anesthesiologists Task Force on Neuromuscular Blockade was published in the January 2023 issue of Anesthesiology. The publication adds the ASA to a growing consensus of societies recommending quantitative over qualitative neuromuscular monitoring [1].
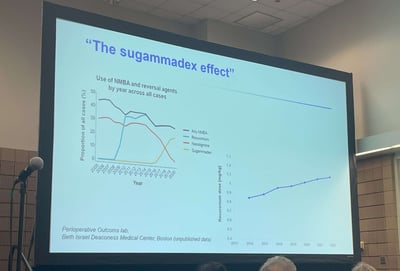
Contrary to the common misconception that sugammadex has eliminated the clinical need for quantitative train of four monitors, utilization of quantitative neuromuscular monitoring is critical to implement the evidence-based recommendations outlined in the guidelines.
As stated by the ASA practice guidelines first author, Dr. Stephan Thilen,
The ASA neuromuscular monitoring guidelines define clinically relevant levels of neuromuscular blockade and include recommended antagonism for each level, providing concrete guidance for the creation of reversal protocols or decision support guides, such as rocuronium reversal guide below, which is supplied to all TwitchView train of four monitor users to aid monitor utility.
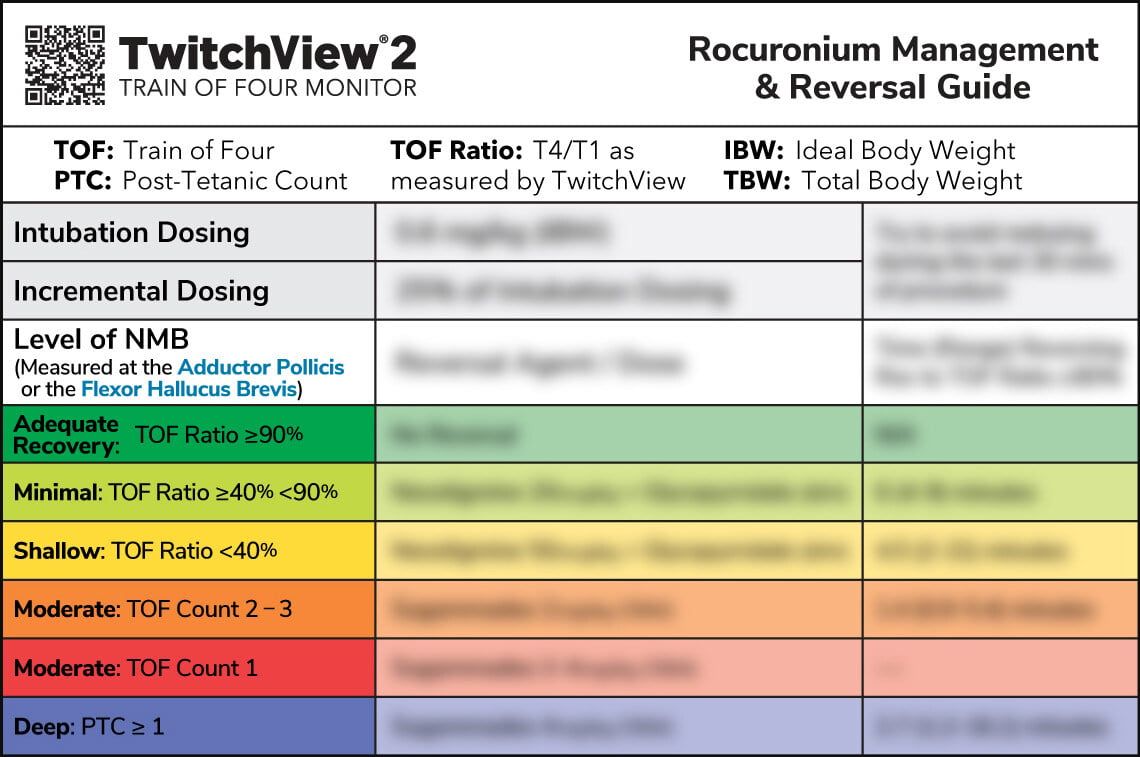
Of note, the recommendations include the appropriate use of neostigmine and abstention of pharmacological reversal if the patient has spontaneously recovered to a TOF ratio ≥90% —made possible by quantitative neuromuscular monitoring.
While quantitative monitoring provides more accurate data than subjective assessments, the onus to implement this data into clinical practice and realize the patient safety benefits remains with the clinician. To avoid residual neuromuscular blockade, the following practice is key:
Confirm a TOF ratio greater than or equal to 0.9 at the adductor pollicis before extubation.
Beyond confirmation of adequate recovery, early adopters of quantitative neuromuscular monitoring like Dr. Thilen have found that they are able to alter neuromuscular blockade management using the continuous data provided by quantitative monitors [2, 3].
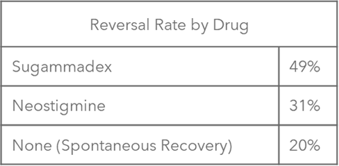
Figure 1: The overall utilization rate for reversal modalities in Dr. Thilen's research.
Practice adjustments include administration of smaller neuromuscular blocking agent intubation doses and smaller more frequent intraoperative redoses of 2-5 mg of rocuronium to maintain tighter control, while still preserving optimal surgical conditions. Such reductions in cumulative NMBA use are thought to enable the safe utilization of neostigmine or abstention from pharmacological reversal when the patient spontaneously recovers to a TOF ratio ≥90%, as recommended by the ASA guidelines.
An example of such neuromuscular blockade management is pictured in the TwitchView TOF monitor trend plot below. A 63 y/o patient was undergoing fusion of the anterior cervical vertebra C4-5 with ACDF under microscope. The surgeon requested minimal neuromuscular blockade citing their goal to minimize the patient’s response to surgical stimuli whilst mitigating potential trauma of the recurrent laryngeal and cervical nerves during the anterior dissection.
Using the continuous data from TwitchView and feedback from the surgeon, the anesthesia provider determined a TOF count 3 provided ideal conditions and titrated blockade accordingly. The patient was reversed with neostigmine and a TOF Ratio of 100% was achieved prior to extubation. Blink Device Company, creators of the TwitchView quantitative neuromuscular monitor have developed a suite of educational tools to support customers as they incorporate the monitors into routine care.
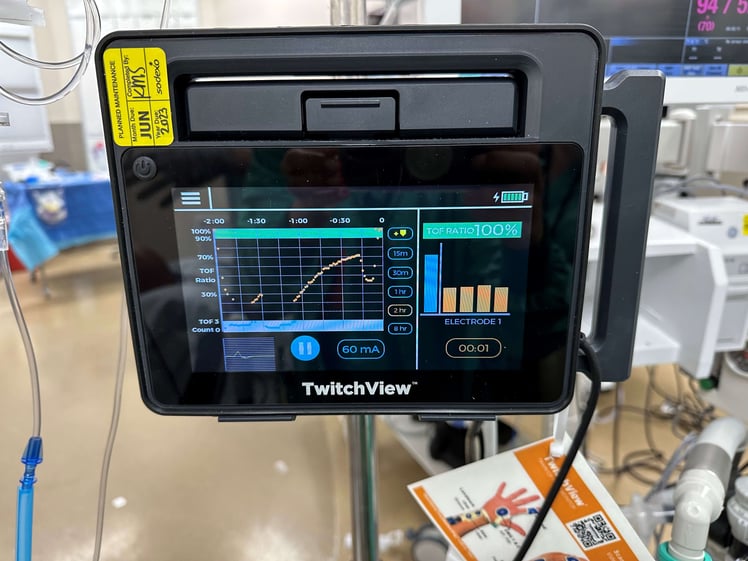 Figure 2: Pictured two-hour trend plot window displaying induction plus 3 maintenance doses of rocuronium and reversal on left and TOF Ratio 100% on right of the TwitchView screen.
Figure 2: Pictured two-hour trend plot window displaying induction plus 3 maintenance doses of rocuronium and reversal on left and TOF Ratio 100% on right of the TwitchView screen.
Understanding that new technology adoption and changes in practice will require time and training, multiple educational opportunities across several different platforms are expected to release in the 2023 calendar year. The following list contains current recommended educational content, and we will share new opportunities as they emerge.
Literature:
Active CME Activities:
Podcasts: