

 Validation in Peer-Reviewed Publications
Validation in Peer-Reviewed Publications
-
Performance Validation: TwitchView EMG is validated as accurate and interchangeable with mechanomyography (MMG) in top-tier publications.4, 5
-
Clinical Validation: TwitchView use has been proven to eliminate residual paralysis and change the management of NMB drugs, enhancing patient safety and reducing unnecessary hospital expenses.1
Convenient Workflow
-
User Interaction: Attach the electrode and press play to start monitoring… that’s it.
-
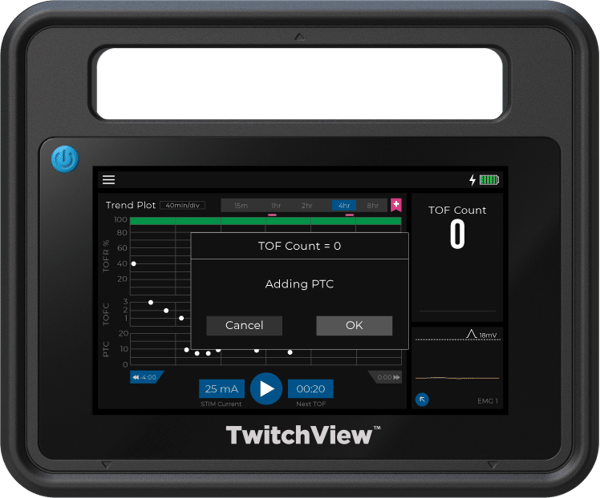
Automatic Monitoring: Patented AutoPTCTM mode automatically switches between TOF and PTC measurements.
-
EMR Connectivity: Eliminates manual charting in Epic, Cerner, Innovian & more. We support an open interface commitment meaning we will connect to any EMR.

Dependable Hardware
-
System Construction: Ruggedized monitor case and cable with a hospital-grade power cord.
-
Universal Mount: Proprietary mounting arm with flexible configurations to support any OR setup.
-
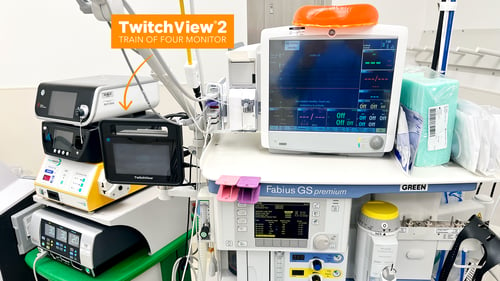
Made in USA: TwitchView2 was designed and built in Seattle, WA
 Advanced Algorithm
Advanced Algorithm
-
EMG Measurement Technique: Performs a comprehensive waveform analysis over thousands of data points, integrating the area under the curve (AUC) of the compound action potential alongside detection of multiple EMG signal features, to precisely identify even the smallest muscle twitches.
-
Noise Cancellation: Isolates the patient signal, capturing waveforms as small as 0.2 mV enabling reliable performance during deep block and in difficult-to-monitor patients like neonates.



New & Improved Electrodes
-
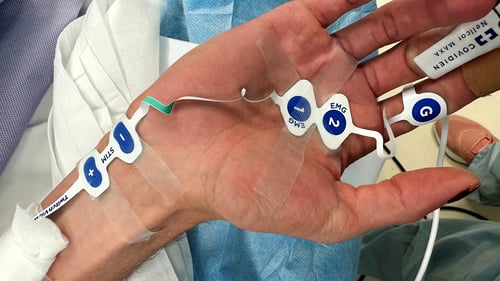
Three electrode sizes: Large, Medium and Small, a neonate-specific electrode for infants <10kg.
-
All sizes are designed with a minimal footprint for placement alongside lines and other sensors.









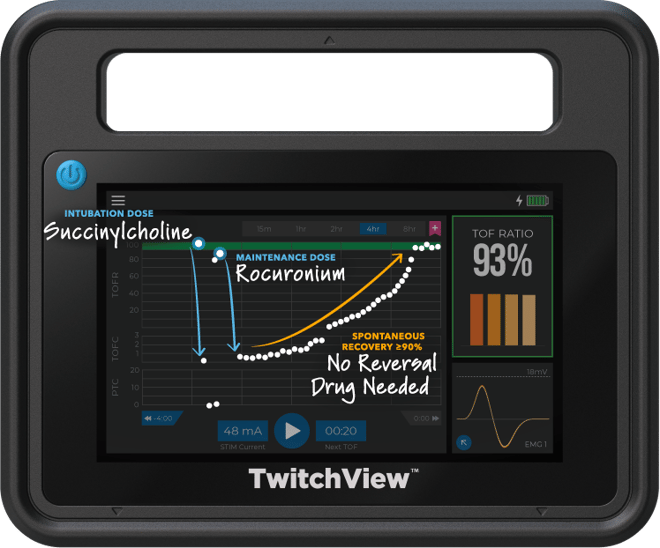
Case Type: Gastrectomy
Case Duration: 4 hours
Patient Age: 35 years
Patient Weight: 148kg
---
Electrode Size: Large
Intubation Dose: 100mg Succinylcholine
Maintenance Dose: 30mg Rocuronium
Reversal: Spontaneous Recovery
TwitchView confirms complete spontaneous recovery to a TOF Ratio ≥90%—no pharmacological reversal needed!

Case Type: Cholecystectomy
Case Duration: 2 hours
Patient Age: 87 years
Patient Weight: 87kg
---
Electrode Size: Large
Intubation Dose: 50mg Rocuronium
Maintenance Dose: 10mg Rocuronium
Reversal Dose: 200mg Sugammadex
After sugammadex administration, it took six minutes to start taking effect and 10 minutes to achieve adequate recovery (TOFR ≥90%). Two minutes after sugammadex was administered, the provider noted four twitches on the face, whereas TwitchView measured a TOF Count (TOFC) 1.
TwitchView accurately informed the provider, preventing this at-risk elderly patient from being extubated at a TOFC 1.

Case Type: Cardiac Catheterization
Case Duration: 2 hours
Patient Age: 12 years
Patient Weight: 34kg
---
Electrode Size: Medium
Intubation Dose: 34mg Rocuronium
Maintenance Doses: 2x 10mg Rocuronium
Reversal: Spontaneous Recovery
Continuous data and the trend plot inform providers of the rapid clearance of rocuronium guiding more frequent dosing. When the case is complete, TwitchView confirms spontaneous recovery was achieved, and no reversal was administered.

Case Type: Congenital Heart Defect Correction
Case Duration: 7 hours
Patient Age: 5 years
Patient Weight: 16.6kg
---
Electrode Size: Medium
Intubation Dose: 2mg/kg Rocuronium (Roc)
1st Maintenance Doses: 4x 0.6mg/kg Roc
2nd Maintenance Dose: 1mg/kg Roc
Reversal Doses: 2x 4mg/kg Sugammadex
Before bypass, TwitchView guided 0.6 mg/kg redoses every 40 minutes to maintain necessary surgical conditions. After 4 mg/kg sugammadex was administered at a PTC of 5, TwitchView indicated recovery had stalled and a second reversal dose was administered.

Case Type: Cleft Palate Repair
Case Duration: 4 hours
Patient Age: 7 months
Patient Weight: 6.7kg
---
Electrode Size: Small
Intubation Dose: 1mg/kg Rocuronium (Roc)
Maintenance Dose: None
Reversal: Spontaneous Recovery
TwitchView indicated that the induction dose of rocuronium provided sufficient surgical conditions in a 4.5-hour case and confirmed spontaneous recovery—no reversal administered.

Case Type: Pyeloplasty
Case Duration: 2 hours
Patient Age: 2 months
Patient Weight: 6kg
---
Electrode Size: Small
Intubation Dose: 1.2mg/kg Rocuronium (Roc)
Maintenance Dose: None
1st Reversal Dose: 4mg/kg
2nd Reversal Dose: 2mg/kg in PACU
4mg/kg reversal dose of sugammadex stalled at a TOFR 42%, but patient passed subjective assessment was extubated and brought to PACU. Recovery did not progress and baby was inconsolable. An additional 2 mg/kg sugammadex was administered in the PACU and baby recovered to TOFR 91%, calmed and accepted a bottle.

