
What is post-tetanic count PTC? Using PTC to proactively manage neuromuscular blockade and ensure optimal surgical conditions during general anesthesia.
It is a familiar moment in the operating room.
The case is ending. Ventilator settings are minimal. The patient is breathing. You stimulate the ulnar nerve and feel the twitches with your fingers. Everything seems reassuring. Four twitches. No obvious fade. The patient lifts their head and may even squeeze your hand or begin bucking.
It feels like they are ready.
So you extubate.
For decades, anesthesiologists have relied on subjective assessment of neuromuscular recovery. This includes tactile or visual evaluation of the train-of-four response and clinical signs such as head lift, tidal volume, or grip strength. These bedside checks are quick, intuitive, and deeply ingrained in anesthesia culture.
But there is a problem.
Our fingers are not very good monitors.
Sometimes the first sign of that limitation appears only after extubation. Oxygen saturation begins to drift downward. The patient coughs repeatedly but cannot effectively clear their airway. Respiratory effort is present, yet ventilation is not quite adequate. Something is not right.
The issue is simple. Human perception is not sensitive enough to detect small differences in neuromuscular transmission.
This limitation has been recognized in neuromuscular monitoring research for more than four decades.
Multiple studies have demonstrated that clinicians cannot reliably detect fade once the train-of-four ratio exceeds approximately 0.4.¹ ² Above that level, four twitches may appear equal even though substantial neuromuscular weakness remains.
In practical terms, a patient with a TOF ratio anywhere between roughly **0.4 and 1.0 may appear identical when assessed qualitatively. **¹ Current anesthesia practice guidelines recommend confirming a train-of-four ratio ≥0.9 prior to extubation to ensure adequate recovery of neuromuscular function.³
Without objective monitoring, extubation decisions often occur within a wide physiologic blind zone between a TOF ratio of 0.4 and 0.9, where subjective assessment cannot reliably distinguish partial recovery from full recovery.
The clinical consequences are not theoretical. Residual neuromuscular blockade remains common when recovery is not objectively confirmed prior to extubation.
This explains a paradox many clinicians have experienced. A patient appears ready based on tactile twitch assessment and other clinical signs, but behaves as though they are partially paralyzed after extubation.
What feels like full recovery frequently is not.
The clinical signs traditionally used to judge recovery, such as tidal volume, sustained head lift, or hand grip strength, are unreliable indicators of neuromuscular recovery. Patients may perform these tasks even when the train-of-four ratio remains well below levels associated with safe airway protection and normal respiratory function. ⁵
These bedside signs reflect recovery of peripheral skeletal muscle strength, not necessarily recovery of the upper airway and respiratory muscles responsible for maintaining airway patency and effective ventilation.
This disconnect between clinical appearance and physiologic recovery is what makes residual blockade difficult to recognize.
The patient may look recovered. The physiology says otherwise.
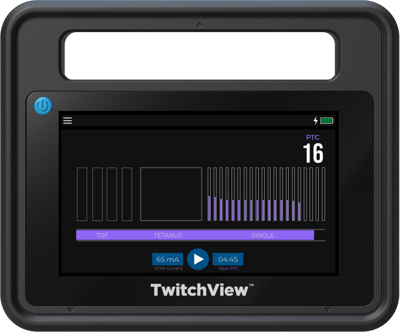
The monitor image below comes from a real intraoperative case.

The patient received 50 mg of Rocuronium at induction, with no additional neuromuscular blockade administered during the procedure. As the case was concluding, 100 mg of Sugammadex was administered at a train-of-four count of three.
Following reversal, the patient began to demonstrate reassuring clinical indicators commonly used to judge readiness for extubation. Spontaneous tidal volumes were present. End-tidal CO₂ was appropriate. The patient demonstrated head lifting, bucking, and purposeful movement.
From a qualitative perspective, the patient appeared ready, but the quantitative monitor showed something different.
At the moment of extubation, the train-of-four ratio was only 39 percent.
This patient was extubated at less than half of the recovery threshold that current anesthesia guidelines recommend.
The patient was followed to the PACU, where jaw thrust and supplemental oxygen were required to maintain adequate oxygen saturation and their PACU stay was extended.
This example illustrates a central limitation of subjective monitoring. Clinical signs of recovery can appear long before neuromuscular transmission has fully recovered.
Without quantitative monitoring, that difference would remain invisible.
Clinical signs of strength often return well before full neuromuscular recovery.
Tasks commonly used to judge readiness for extubation require only partial restoration of neuromuscular transmission.
Ali and colleagues demonstrated that patients could perform sustained head lift and generate apparently adequate respiratory parameters despite incomplete recovery from neuromuscular blockade.⁵
Viby-Mogensen and colleagues later showed that commonly used clinical tests of strength are poor predictors of adequate neuromuscular recovery.¹
These findings helped establish the recovery threshold now widely accepted in anesthesia practice.
Upper airway muscles and protective airway reflexes recover more slowly than peripheral muscles, which is why a train-of-four ratio ≥0.9 is recommended before extubation.³
Below that level, patients may breathe, move, and follow commands while still having impaired airway protection and reduced ventilatory reserve.
The patient may appear recovered while the physiology tells a different story.
This is the gap that quantitative neuromuscular monitoring reveals.
The monitor image below captures another emergence scenario.

The patient received 40 mg of Rocuronium at induction. Later in the case, after spontaneous recovery to a train-of-four count of one, an additional dose of neuromuscular blockade was administered. As the procedure approached completion, reversal was initiated with Neostigmine and Glycopyrrolate. During emergence, the quantitative monitor demonstrated persistent residual blockade with a train-of-four ratio of 32 percent. An additional 2 mg of Neostigmine was administered.
Recovery progressed and the patient was extubated when the monitor showed a train-of-four ratio of 70 percent.
From a qualitative standpoint this stage of recovery can appear reassuring. Four twitches may be present and fade is difficult to detect by touch or visual assessment.
The quantitative monitor reveals something different. Recovery is progressing, but neuromuscular transmission has not yet returned to normal.
When recovery is judged subjectively, the difference between partial recovery and full recovery can be difficult to detect.
Objective monitoring makes that difference visible.
The disconnect between perceived recovery and true neuromuscular recovery has been documented in anesthesia literature for decades.
Viby-Mogensen and colleagues demonstrated that **residual neuromuscular blockade was present in a substantial proportion of patients arriving in the PACU following routine anesthetic care.**¹
Baillard and colleagues later reported that **approximately 42 percent of patients arriving in the PACU had residual neuromuscular blockade when objective monitoring was not routinely used.**⁶
Residual blockade is not merely a laboratory finding. Murphy and colleagues demonstrated that **patients with residual neuromuscular blockade were significantly more likely to experience critical respiratory events in the PACU, including hypoxemia and airway obstruction.**⁴
These findings helped shape modern anesthesia practice recommendations.
An international consensus panel on neuromuscular monitoring concluded that **quantitative monitoring should be used whenever neuromuscular blocking drugs are administered and that subjective assessment alone is insufficient to confirm recovery.**⁷
These recommendations did not emerge because clinicians lack experience or skill. They emerged because human perception has inherent limits when evaluating neuromuscular transmission.
When clinicians rely solely on tactile or visual assessment, recovery may appear adequate while meaningful blockade persists. Quantitative monitoring does not change the physiology of neuromuscular recovery - It changes visibility.
Neuromuscular blockade does not recover in steps we can feel. It recovers along a physiologic curve. Quantitative monitoring simply allows clinicians to see where the patient actually is on that curve.
And when the decision is whether a patient can safely breathe, protect their airway, and maintain ventilation, seeing that curve matters.


